
")
Etiological Background
Dehydration is a medical condition, resulting in the progressive depletion of bodily fluids. The total body water content decreases due to fluid losses exceeding fluid replacement. This process mostly occurs in the body’s main organ systems, including: skin, lungs, kidneys, and gastrointestinal tracts. Multiple forms of dehydration exist, however the majority of physical fluid loss can be broken down into three main categories. Isotonic dehydration occurs when equal parts water and sodium have been lost. Hypotonic dehydration is caused due to a primary loss in sodium. Conversely, hypertonic dehydration refers to water losses exceeding sodium levels. Having established this distinction, it is necessary to clarify that the discussion will specifically focus on isotonic dehydration from the skin. Isolating these conditions is due to the bodily and environmental factors surrounding them. Specifically, with regards to excess water loss from the skin; the most common attributors are heat and exercise. Additionally, isotonic dehydration can be caused by excessive sweating. [1-2] All three factors are present in the context of athletes and specifically, active soccer players.
Context
It is possible for any demographic to exhibit the adverse effects of dehydration when the necessary conditions are met. However, there are select groups more prone to risk than the average healthy human with a body water content of 60%. [3] It has been widely documented that an athlete’s optimal performance is impaired, to a certain capacity, by dehydration. This observation is validated with respect to endurance-based exercises that incorporate repeated isotonic contractions of large muscle groups. [4-5]
A subset of the previously identified, endurance-based, athlete group is soccer players. In contemporary culture, soccer is one of the most influential sports in the world. Performed by adults and children alike, the sport tests the user’s capacity in both psychological and physiological areas. With regards to actions, players typically run about 10km during the duration of a 90 minute match. However, during that sequence of time, they also perform a series of about 1,000 mini actions which include: sprints, slide tackles, headers, passes, movement with the soccer ball. These actions require a level of intensity, typically measured through maximal heart rate. Performing aerobic movement for the entire duration of a soccer match is the equivalent to a soccer player approaching the limits of anaerobic intensity. This could be quantified as utilizing up to 90% of their maximal heart rate. [6]
Dehydration in Soccer
It has been proposed that dehydration impedes on the quality of a player’s performance and that the only way to maintain homeostasis during a match is through adequate hydration. However, whether dehydration is influencing performance based on a psychological or physiological scale remains equivocal. Additionally, there is equal ambiguity with regards to the degree of influence dehydration has on said scales. Therefore, evaluations of both the psychological and physiological conditions, individually and in concert, remain necessary.
Psychological Condition
It is possible that a player’s decrease in performance is rooted within the negative psychological associations between dehydration and comfort. Restriction of fluid intake and its resulting physical side effects (e.g. thirst) modulate a player’s perceived exertion to a higher degree. That greater exertion suggests to the player that the game is also of a greater difficulty. The result is a behavioral change including an increased desire to drink and/or a decline in physical intensity. [7-8] It has been documented that the amount of high intensity movements and distance covered drops from the first 45 minute half to the second of a match. [6] It’s possible this disparity is due in part to the behavioral shifts previously mentioned.
However, loss of optimal performance can be reduced in the later stages of a match. When the desire to drink is fulfilled, it alleviates the thirst mechanism. It is unclear whether fluid ingestion during this period is purely a psychological enhancement or also assists the physical needs of a player. The reason being, the process of ingestion to changes in osmosis averages between 40-60 minutes. [9] This would suggest that the physical benefits do not take effect until post-match. Therefore the greatest effect fluid intake serves during a match is likely a reduction in perceived difficulty and in turn perceived exertion.
Physiological Condition
The large number of variables in soccer makes it difficult to obtain accurate and reproducible data. This is due largely to the complexities of player movements and the external circumstances surrounding the game. However, this evaluation focuses specifically on body mass which will serve as a single dehydration examination method example for other physical factors (e.g. sweat loss, urine concentration, plasma osmosis, temperature conditions) and their capacity to assess hydration. Furthermore there will be a brief overview on the physical nuance of fluid intake.
Related to body mass, fluid loss can be assessed through the rapid changes in a player’s body mass percentage, pre and post-match. It is typical to lose 1 to 2% of body mass during a competitive soccer match. Percentages vary depending on the context of the match. However, assuming that environmental conditions are fair and there is minimal opportunity to drink, this average remains true. Additionally, when evaluating a player’s long term hydration status, body mass can serve as a sufficient marker. Over several week periods, more acute changes in mass will occur due to the law of Large Numbers. The result is a more reliable measuring tool than observing shifts in total body water content. Alternatively, long periods of evaluation also allows for the inclusion of shifts in fat and lean mass which influence total body mass and differ from bodily water mass. [10]
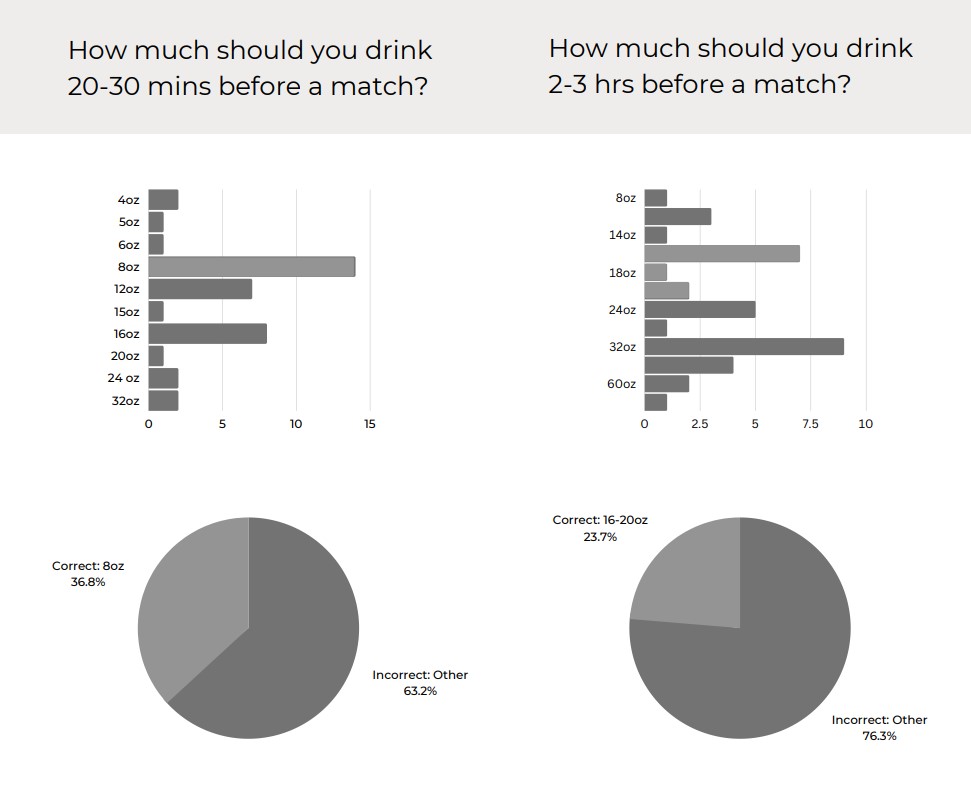
Proper fluid intake preceding a match is considered equal if not more crucial than fluid intake during a match to achieving homeostasis. It has been widely cited that 20 to 30 minutes before exercise, a player should consume 8 fluid oz. This is in addition to the 16 to 20 fluid oz needed 2 to 3 hours prior to the match. [11] Despite access to such knowledge, a considerable portion of soccer players are already dehydrated just prior to their match.
Intersection of Conditions
Discrepancies in soccer player’s hydration status are apparent in both the physical and psychological space. However, it’s unlikely that one variable operates completely independent of the other. For this reason, primary research was conducted on comparing reported fluid consumption with perceived fluid consumption and fluid intake knowledge. The basis of the study was rooted in a 10 question survey and a series of ethnographic style observations. The survey population included the participation of active collegiate and high school level soccer players.
Of the 38 participants, 71.1% reported having prior knowledge on hydration. In spite of this perception, only 30.25% of respondents answered the knowledge based questions correctly. This discrepancy between apparent knowledge and actual knowledge differed by about 41%.
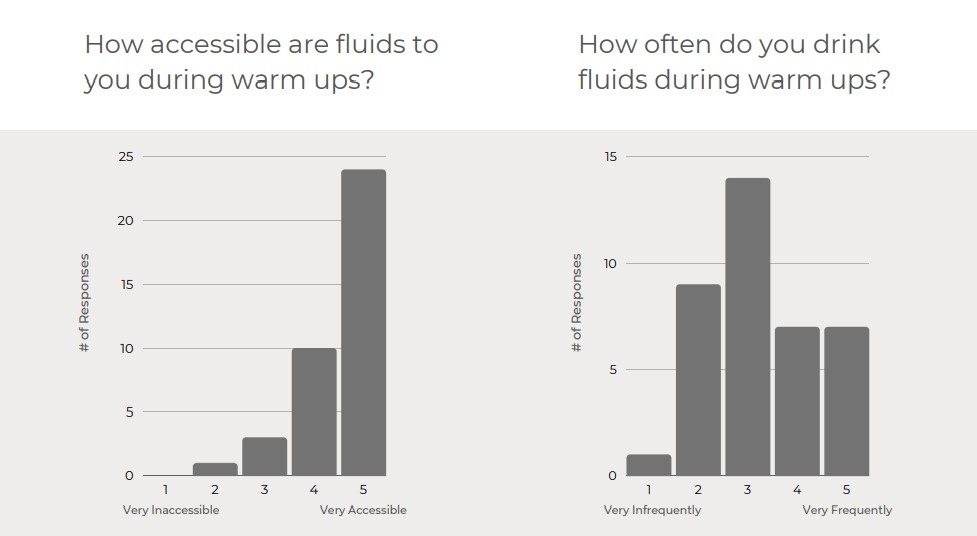
Drinking behavior was measured in relation to accessibility to fluids. Despite a positive association between player perception and fluids being easily accessible, there was a more evenly distributed spread of players who reported or were observed being adequately hydrated.
These insights reveal that improper fluid intake is a larger, multifaceted issue. It is determined by a player’s ability to discern proper information on hydration and the manner in which they apply that knowledge.
Conclusion
Considering the array of intricate components associated with hydration and soccer, it is improbable that a single psychological or physiological factor serves as the sole attributor for dehydration-based decline in performance. A more plausible scenario is that dehydration is a single factor amongst an interconnected system that alters psychological stimulus within the player. That mental shift influences the player’s mental capacity and perception on performing the actions necessary in soccer. This, in turn, results in the player making physical adjustments in an effort to accommodate the strain.
Based on that scenario, the design objective becomes clear: develop a product that physically intervenes during the beginning stages of a soccer player’s fatigued state; prolonging or mitigating the psychological burden and the side effects that arise in turn.
References
- Weinberg, A. D., & Minaker, K. L. (1995). Dehydration. Evaluation and management in older adults. Council on Scientific Affairs, American Medical Association. JAMA, 274(19), 1552–1556. https://doi.org/10.1001/jama.274.19.1552
- Thomas, D. R., Cote, T. R., Lawhorne, L., Levenson, S. A., Rubenstein, L. Z., Smith, D. A., Stefanacci, R. G., Tangalos, E. G., & Morley, J. E. (2008). Understanding clinical dehydration and its treatment. Journal of the American Medical Directors Association, 9(5), 292–301. https://doi.org/10.1016/j.jamda.2008.03.006
- Shaheen, N. A., Alqahtani, A. A., Assiri, H., Alkhodair, R., & Hussein, M. A. (2018). Public knowledge of dehydration and fluid intake practices: variation by participants’ characteristics. BMC public health, 18(1), 1346. https://doi.org/10.1186/s12889-018-6252-5
- Montain, S. J., & Coyle, E. F. (1992). Influence of graded dehydration on hyperthermia and cardiovascular drift during exercise. Journal of applied physiology (Bethesda, Md. : 1985), 73(4), 1340–1350. https://doi.org/10.1152/jappl.1992.73.4.1340
- Morici, G., Gruttad’Auria, C. I., Baiamonte, P., Mazzuca, E., Castrogiovanni, A., & Bonsignore, M. R. (2016). Endurance training: is it bad for you?. Breathe (Sheffield, England), 12(2), 140–147. https://doi.org/10.1183/20734735.007016
- Stølen, T., Chamari, K., Castagna, C. et al. Physiology of Soccer. Sports Med 35, 501–536 (2005). https://doi.org/10.2165/00007256-200535060-00004
- Abbiss, C.R., Peiffer, J.J., Meeusen, R. et al. Role of Ratings of Perceived Exertion during Self-Paced Exercise: What are We Actually Measuring?. Sports Med 45, 1235–1243 (2015). https://doi.org/10.1007/s40279-015-0344-5
- St Clair Gibson, A., Lambert, E. V., Rauch, L. H., Tucker, R., Baden, D. A., Foster, C., & Noakes, T. D. (2006). The role of information processing between the brain and peripheral physiological systems in pacing and perception of effort. Sports medicine (Auckland, N.Z.), 36(8), 705–722. https://doi.org/10.2165/00007256-200636080-00006
- —
- Cheuvront S.N., R. Carter III, S.J. Montain, and M.N. Sawka (2004). Daily body mass variability and stability in active men undergoing exercise-heat stress. Int. J. Sport Nutr. Exerc. Metab. 14: 532-540.
- SportsMedBC. (2021). Fluid first-hydration in sports. SportMedBC. Retrieved October 2, 2022, from https://sportmedbc.com/article/fluid-first-hydration-sports



{kind=link}